
People with patellofemoral pain commonly present movement patterns impairments during functional activities.1 Additionally, the higher number of movement patterns impairments is associated with higher self-reported pain and poor functional capacity.2
Therefore, it is recommended that therapists carefully assess the movement patterns throughout the kinetic chain during different tasks, mainly those that exacerbate patient symptoms, as identified biomechanical deficits may indicate a more severe condition and can help guide an individual-specific treatment plan.
Functional performance tests that simulate daily activities have been proposed to facilitate such analysis. In this section, you will find some alternatives to assess movement patterns in the clinical setting.
Identification of altered movement patterns of a patient with patellofemoral pain might aid in the therapist’s selection of appropriate rehabilitation, which may include movement retraining. The current “gold standard” for analyzing movement patterns is three-dimensional (3D) motion analysis. However, the cost and expertise required to obtain accurate and reliable data with 3D motion analysis make it less feasible for use in the clinical setting. Possible alternatives for the clinical setting include two-dimensional (2D) motion analysis using a video camera and/or visual observation.
Some practical tips to improve video analysis or visual observation are:
1. Position the camera statically, always at the same height and distance from the person to be evaluated.
2. If possible, place at least one camera in front and one on the side of the patient, as people with patellofemoral pain may have movement impairments in both planes (frontal and sagittal).1
3. The addition of markers in specific body landmarks, such as the center of patella, ASIS, lateral malleolus may help identify altered movement patterns.
The forward step-down test is a reliable functional test3 that simulates, in the clinical environment, the activity of going downstairs, increasing the load on the knee at different flexion angles, as well as dynamic muscle control. Participants should stand on a platform or a step in a bipedal stance and step forward to tap with their non-test leg on the ground in front of the step, while keeping the tested leg on the step, before returning to starting position.
See the video below for further details on how to perform and score the forward step-down test.4
How to perform the test
 How to score
How to score
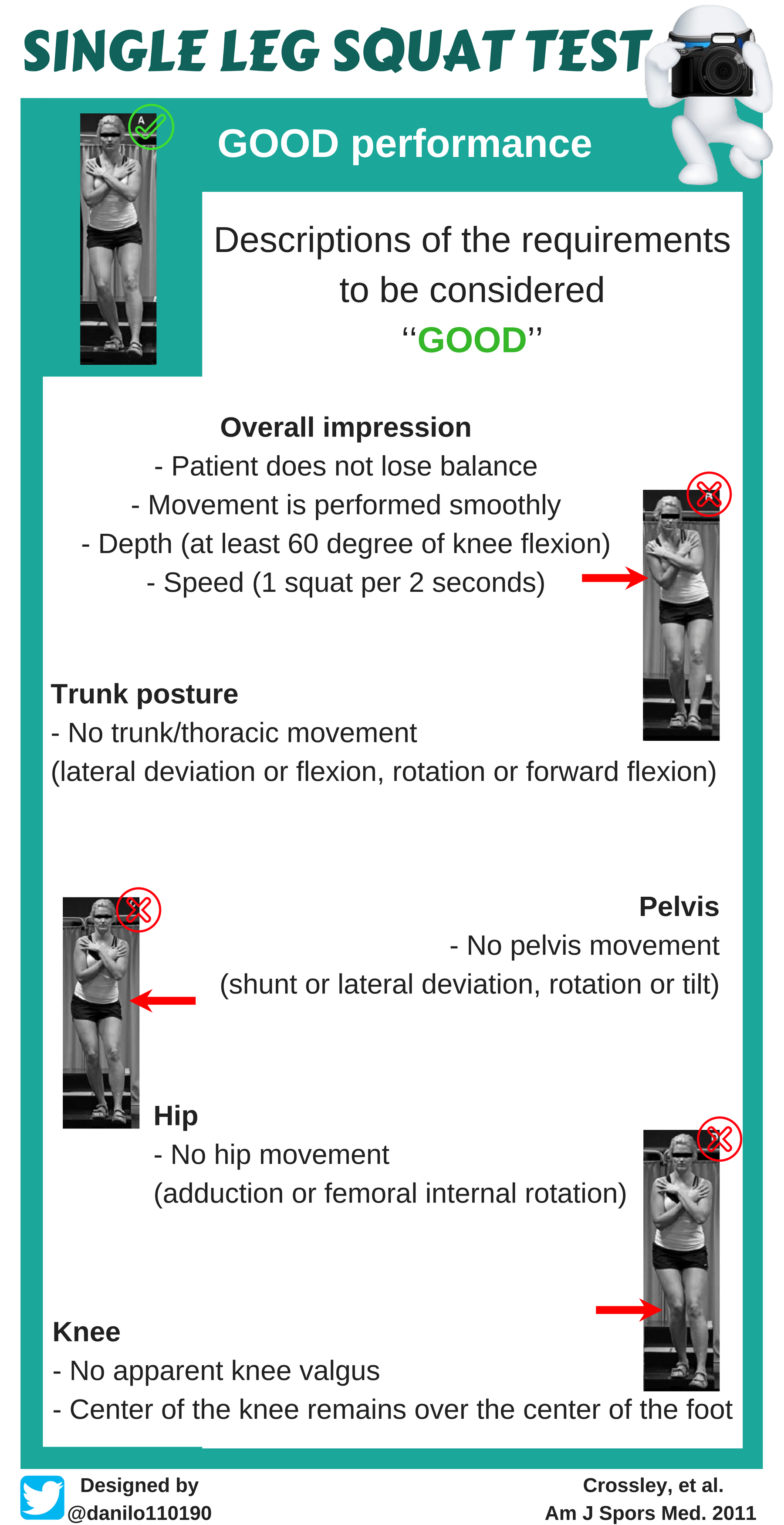
Trunk/thoracic rotation
Trunk/thoracic lateral flexion
Trunk/thoracic forward flexion
Pelvic rotation
Pelvic tilt (take note of the depth of squat)
Hip (femoral) internal rotation
Knee position relative to foot position
Watch the video below with Dr. Neal Glaviano, answering the most common questions about this topic [COMING SOON]:
Now that you have reviewed everything about clinical assessment of movement patterns of people with patellofemoral pain, test your knowledge by taking the quiz below.
References
- Powers et al. 2017. Evidence-based framework for a pathomechanical model of patellofemoral pain: 2017 patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester, UK: part 3.
- Ferrari et at. 2018. Higher pain level and lower functional capacity are associated with the number of altered kinematics in women with patellofemoral pain.
- Loudon et al. 2002. Intrarater Reliability of Functional Performance Tests for Subjects With Patellofemoral Pain Syndrome.
- Park et al. 2013. Musculoskeletal predictors of movement quality for the forward step-down test in asymptomatic women.
- Crossley et al. 2011. Performance on the single-leg squat task indicates hip abductor muscle function.